

The billing process requires two distinct approaches if you receive medical treatment in a doctor’s office or hospital. Understanding the difference between physician and hospital billing is important because it directly influences how healthcare providers are paid, how claims are processed, and what appears on your bill.
These billing techniques operate under different rules, utilize various forms and have distinct reimbursement models. Understanding these distinctions is crucial to maintaining financial stability and compliance for medical and clinic administrators and billing professionals.
Physician billing, also known as professional billing, is a term used to describe services provided by individual healthcare providers who are not hospitals. Imagine your routine check-up at your family practice, a specialist consultation or physical therapy provided by an independent clinic. These visits generate professional invoices detailing what the practitioner did.
The billing process is based on the direct care provided by the doctor–examination and diagnosis, treatment choices and medical guidance. When your doctor reviews symptoms, orders diagnostic tests, or formulates the treatment plan, these services are translated into codes that insurance companies can recognize.
Professional billing is heavily based on management and evaluation codes, commonly called E/M codes. They range from 99202 to 99499 and reflect the complexity of medical decision-making and the time spent during interactions. A simple follow-up visit will be coded differently from a more complicated consultation requiring thorough medical history reviews.
Hospital billing, often called institutional billing, has an extensive scope. If you’re admitted to surgery, stay in an emergency room or receive outpatient care in a hospital-affiliated clinic it triggers a different billing process.
This type of billing records the doctor’s actions and includes facility costs for operating rooms and medical equipment, nursing care, the medications that were administered, and laboratory work. The bed you were in. Every item is processed by an enormous database known as the charge master.
The charge master is the hospital’s complete pricing catalog that lists the various services offered by the hospital from 20,000 to 50,000. Each entry contains department codes and charge codes, as well as descriptions, and prices that form the foundation of the revenue cycle in hospitals.
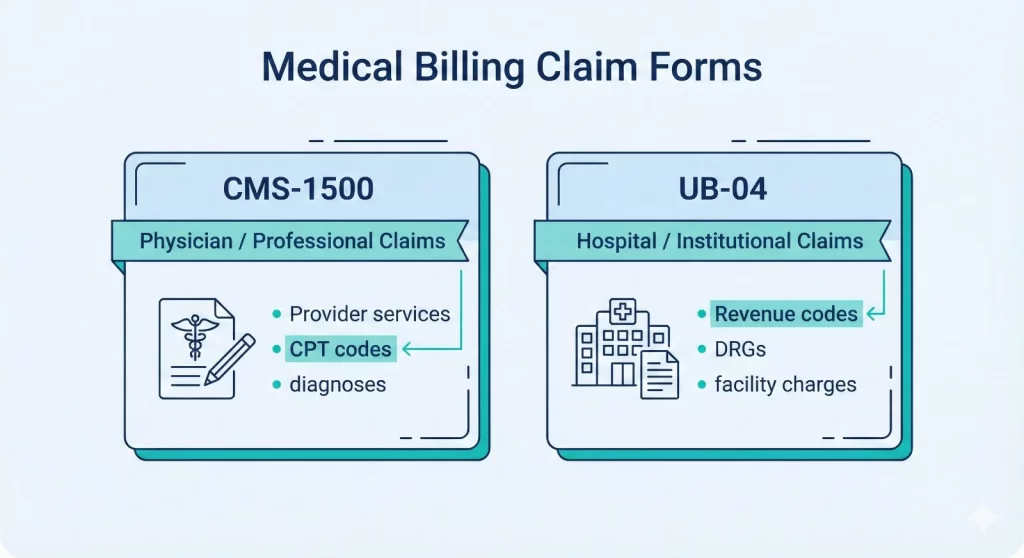
The main distinct feature of physician and hospital billing is the claim forms used. Professional billing utilizes the CMS-1500 form, which was designed for individual practitioners as well as group practices. The form gathers information about the patient’s demographics, diagnosis codes, procedure codes, charges, and other details about the provider.
Hospital billing is handled using the UB-04 form, which is also called CMS-1450. This form for claims by institutions handles hospital services and has fields for several departments, revenue, and condition codes.
Professional claims utilize he format 837-P when electronically submitted, while claims from institutions use the format 837-I. The “P” is for experienced, and the “I” refers to institutional.
Medical Coding systems utilized for physician and hospital billing differ, but they are not identical. Professional billing typically utilizes CPT codes (Current Procedural Terminology) and HCPCS Level II codes to identify services provided.
CPT codes are licensed by the American Medical Association and updated each year. Physicians also use ICD-10-CM codes to document diagnoses and justify why the medically required services are needed.
Hospital billing utilizes the same coding systems, but applies them to a broader range of services. A single hospitalization can include many CPT codes, multiple diagnosis codes, and a myriad of revenue codes that categories the charges according to department.
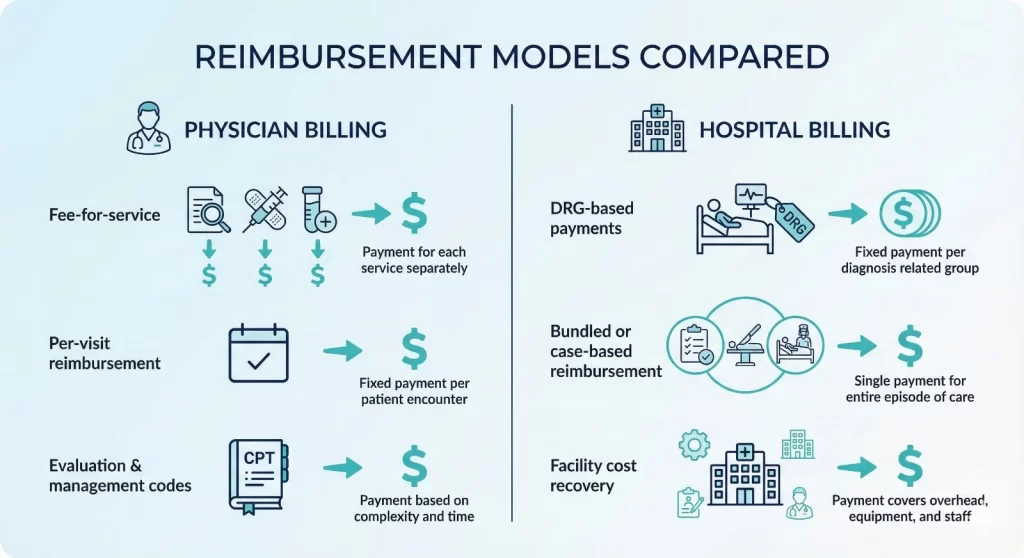
The way that providers are paid determines the quality of healthcare. Most physician billing is a fee-for-service model, where doctors are paid for each service on established schedules the more complicated the visit and the more complex the visit, the greater the reimbursement amount.
Hospital billing utilizes a variety of reimbursement methods, including fee-for-service. Diagnosis-related groups, or DRGs, pay for many hospitals stays. Medicare and other payers assign cases to DRG groups based on the diagnosis of complications, the procedure, and the diagnosis carried out.
The hospital receives a set amount regardless of the duration of stay. If the hospital can manage the case well and efficiently, it will retain the difference. The hospital is responsible for the difference if the cost exceeds the DRG payment.
Certain hospital services employ the bundled payment model, combining several services into a single payment.
Controlling physician billing involves smaller teams that manage specific workflows. Practices typically have billing specialists who know special codes and contracts for payers. Some handle billing internally while others contract out to ease the burden.
Hospital billing is a process that requires separate departments due to the volume and complexity. Multiple healthcare professionals are involved in the cost of a single patient’s bill: doctors, technicians, nurses and therapists all document services. The billing department oversees all inputs and prepares clear claims.
The management of revenue cycles in hospitals entails sophisticated systems that monitor patients from admission to the final payment, integrating medical documentation and charge capture, coding and denial control.
If you’re in a doctor’s office or a hospital setting, understanding how physician billing and hospital billing diverge can help you avoid costly errors. The wrong form for claims is rejected. Services that are not coded correctly can result in denials that require expensive appeals. Hospitals spend $181 per claim for reworking denials, whereas practices spend $25 for each claim.
The stakes are very high. Around 15% of the claims submitted to private payers are denied, with the hospital denial rate ranging from 10%-11%. Many denials can be avoided by understanding the billing requirements, proper documentation, and precise coding.
For doctors who are considering practices owned by hospitals, it is important to understand the implications. Provider-based billing is when patients pay two bills, one professional charge and one facility fee, resulting in a higher out-of-pocket cost.
The healthcare billing landscape is evolving due to technological regulations and demands from payers. Revenue cycle management increasingly relies on automation and artificial intelligence to minimize errors and increase the acceptance of claims.
For professionals in medical billing keeping up-to-date with the latest coding and requirements for documentation is essential. The Centers for Medicare and Medicaid Services regularly change the guidelines for E/M coding and also adjusts payment methods.
In the end, whether you’re navigating physician billing or hospital billing the main goal is precise documentation, an accurate Coding, timely submission of claims and a timely reimbursement. Recognizing these key differences will allow you to maximize financial performance while ensuring the highest standards of care for patients.