Common Denial Category | What it usually means | Denial Prevention that actually works |
Eligibility/coverage | Patient not eligible on DOS, plan mismatch, COB not updated | Verify eligibility same day or day before date of service; Confirm PCP/referral rules; confirm COB/secondary details before claim submission |
Missing/incorrect patient or claim data | Demographics, subscriber ID, NPI, taxonomy, address, DOB, claim, format errors | Standardize intake + claim-build validation; use a “clean-claim” checklist |
No prior authorization (PA) / TAR | Service requires PA/TAR, but none on file—or doesn’t match | Confirm PA requirement before care; ensure the authorization matches code/DOS/provider/location; attach required clinicals for review programs |
Coding / modifier errors | Code pair edits, wrong modifier, mismatch between dx and procedure | Train on common edits; run edit checks; confirm modifier appropriateness; fix patterns by payer/provider, not “one-off” |
Medical necessity / documentation gaps | Notes don’t support the service billed (or payer expects extra docs) | Use payer-specific documentation expectations; make documentation habits consistent; submit supporting records when required |
Non-benefit / coverage limitations | Code is not covered for that plan/setting, or benefit limits exceeded | Verify benefits before care; if appropriate, use plan dispute/appeal pathways with medical necessity documentation |
Provider enrollment / credentialing issues | Rendering/billing provider not enrolled, wrong taxonomy, not active for DOS | Keep credentialing/enrollment current; confirm payer effective dates; monitor re-credentialing and provider file accuracy |

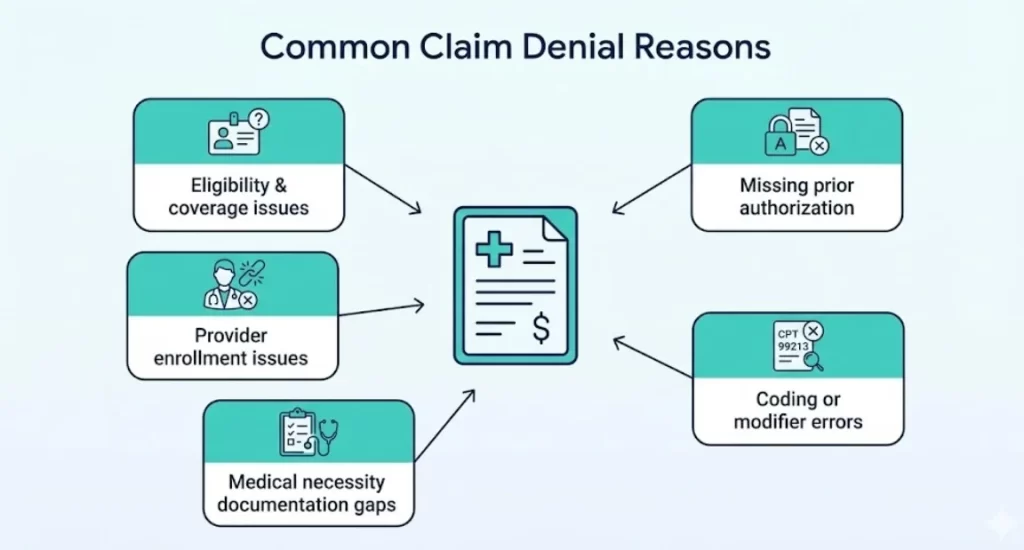 The most common claim denial reasons are eligibility/coverage issues, missing or inaccurate patient/provider data, missing prior authorization, coding/modifier errors, and medical necessity/documentation gaps. To avoid denials, build a simple front-end checklist (verify coverage + benefits, confirm authorization rules, confirm provider enrollment/credentialing, and validate coding/modifiers), then use denial trends from your remits to fix the root cause and not just resubmit.
The most common claim denial reasons are eligibility/coverage issues, missing or inaccurate patient/provider data, missing prior authorization, coding/modifier errors, and medical necessity/documentation gaps. To avoid denials, build a simple front-end checklist (verify coverage + benefits, confirm authorization rules, confirm provider enrollment/credentialing, and validate coding/modifiers), then use denial trends from your remits to fix the root cause and not just resubmit. 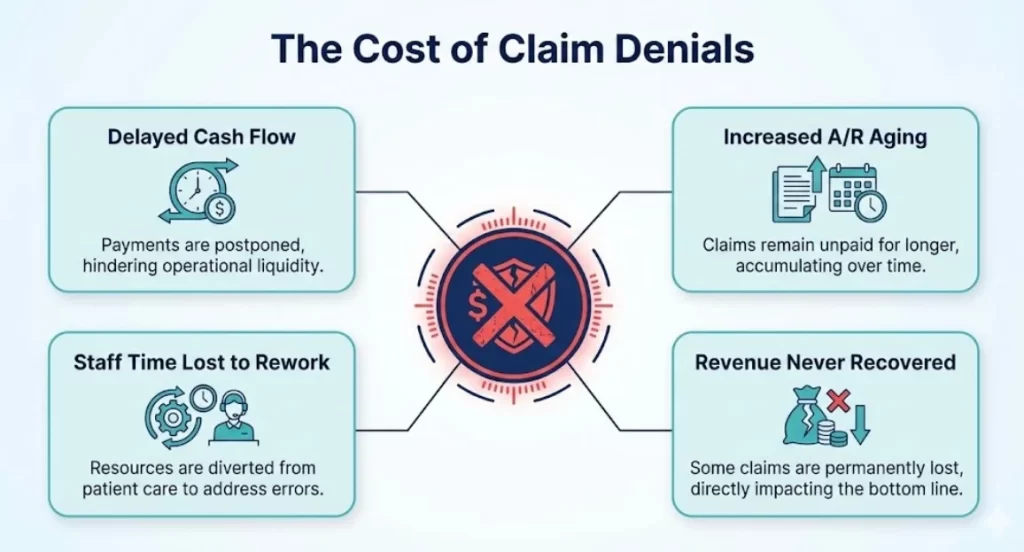 Denials create two kinds of costs:
Denials create two kinds of costs:
