If you are a doula in California, credentialing is not just paperwork. It is the difference between being able to accept Medi-Cal and commercial insurance clients versus having to turn families away or rely only on cash pay. Done right, credentialing turns your calendar into predictable revenue and makes your services accessible to more families.
This guide walks you through
doula insurance credentialing in California, including Medi-Cal enrollment, managed care contracting, common requirements, timelines, costs, and the real world issues that delay approvals.
Quick Answer
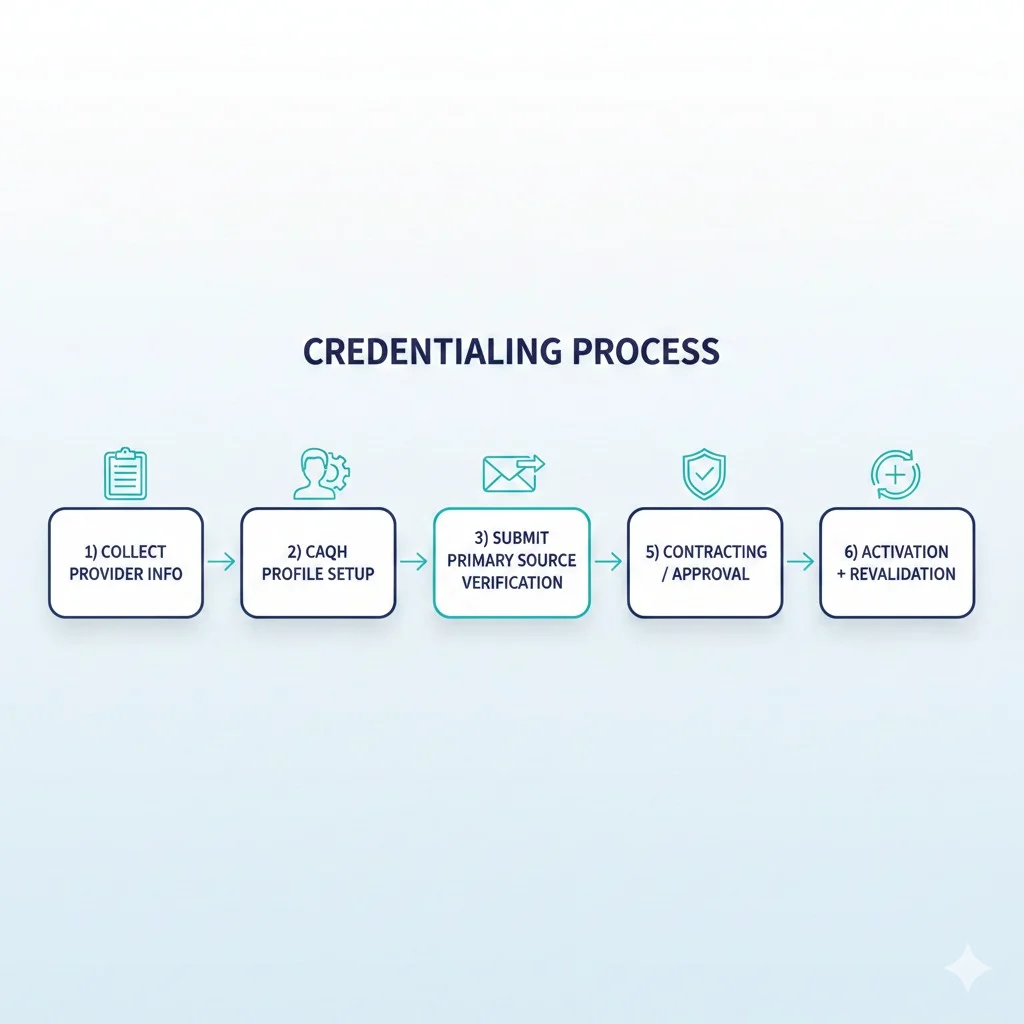
Doula insurance credentialing in California usually starts with Medi-Cal enrollment through DHCS PAVE, then continues with contracting and
credentialing with Medi-Cal managed care plans and any commercial plans that accept doula services. Expect 60 to 120 days for a clean Medi-Cal enrollment in many cases, and another 30 to 90 days per managed care plan once you begin contracting. Your biggest delays typically come from missing documents, business registration items, and confusion between enrollment, credentialing, and contracting. DHCS provides a doula enrollment checklist and a dedicated doula enrollment FAQ, and the Medi-Cal doula manual outlines covered services and billing rules.

 A doula can do everything right clinically and still struggle financially if insurance work is not set up cleanly.
Credentialing impacts:
A doula can do everything right clinically and still struggle financially if insurance work is not set up cleanly.
Credentialing impacts: