If you run a therapy practice, group practice, or outpatient behavioral health clinic in California, insurance credentialing is not “admin work.” It is revenue access.
When credentialing is done right, you can accept the patients who actually want to see you, bill cleanly, and avoid months of claims getting denied because a provider was never correctly linked to the group, location, or payer system. When it is done wrong, it shows up as delayed cash flow, lost sessions, and a front desk stuck explaining why a patient is suddenly out of network.
This guide is written for practice owners and operators who need a clear plan, not a textbook.
What are Mental Health Credentialing Services?
Mental health credentialing services manage the administrative process of vetting a provider’s qualifications (education, license, malpractice history) with insurance companies. In 2025, this process involves two distinct phases: Credentialing (verification) and Contracting (rate negotiation).
- Time to Complete: 90–180 days on average in California.
- Key Portal: PAVE (for Medi-Cal) and CAQH (for private payers like Aetna/Blue Shield).
- Why Use a Service? To prevent revenue delays. A single error on an application can restart the 3-6 month clock, halting your ability to bill.
How Claim N Billing supports mental health credentialing services in California
At Claim N Billing, we treat credentialing like the foundation of your revenue cycle, because it is.
Our credentialing support is designed for busy practice owners who do not have time to chase portals, fix mismatched records, and wonder why claims keep rejecting. We help you get set up cleanly, track every submission, and push applications forward with consistent follow up so you can start billing with confidence.
You can learn more about Claim N Billing and our credentialing focus on our site.
What you can expect when you work with us
- A clear credentialing plan based on your payer goals and practice structure
- Clean setup for providers, groups, and locations before submission
- CAQH build support and ongoing maintenance guidance
- Payer application submission and tracking
- Weekly follow up and status updates
- A practical go live checklist so you are not guessing when to start billing

 Credentialing is the payer’s process of verifying a provider and approving them to participate in a network. Contracting is the agreement and rates. Enrollment is the administrative setup that allows claims to be accepted and paid. These steps overlap, and that is exactly why credentialing feels messy in real life.
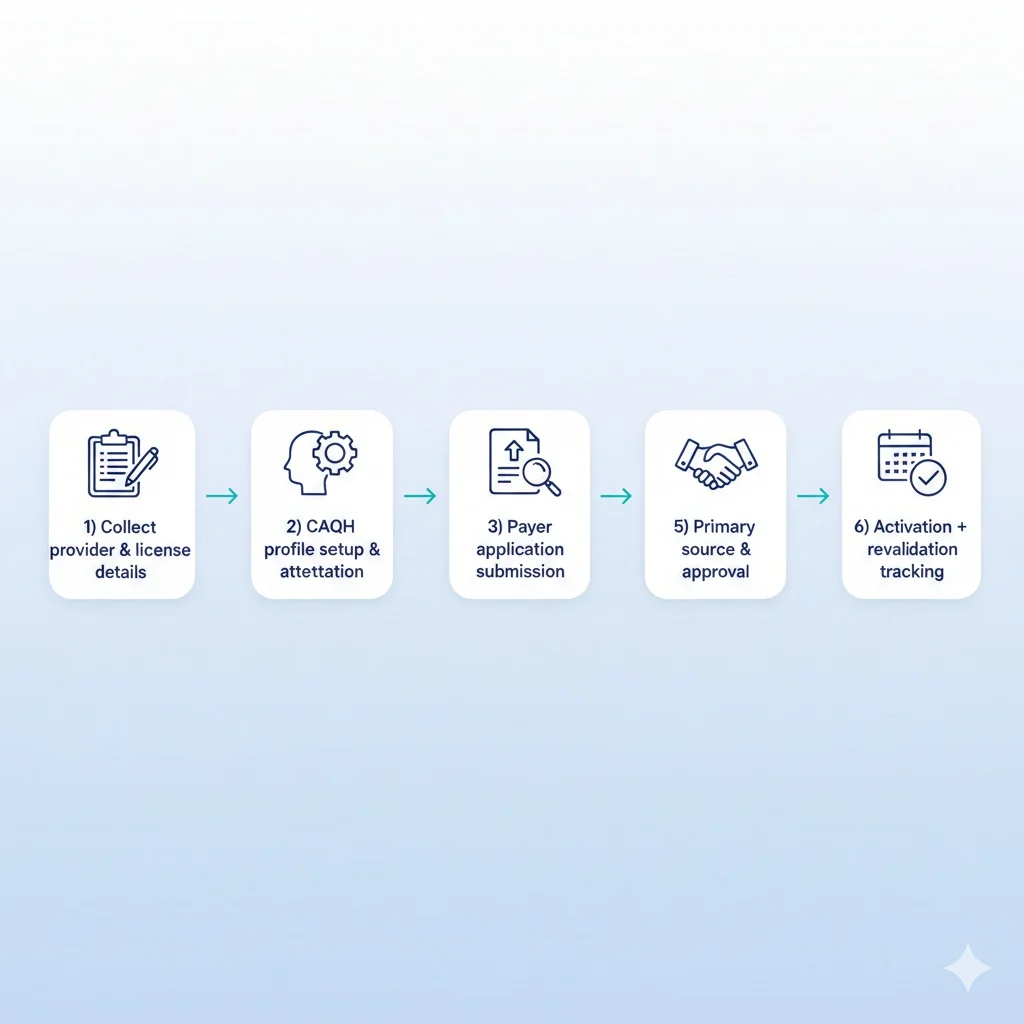
For mental health providers, credentialing typically includes:
Credentialing is the payer’s process of verifying a provider and approving them to participate in a network. Contracting is the agreement and rates. Enrollment is the administrative setup that allows claims to be accepted and paid. These steps overlap, and that is exactly why credentialing feels messy in real life.
For mental health providers, credentialing typically includes:
 Credentialing impacts revenue in very direct ways:
Credentialing impacts revenue in very direct ways: