
Prior Authorization Services
What Are Prior Authorization Services?
Prior authorization (PA) services help clinics obtain insurance approval before certain procedures, imaging, DME, or specialty services are performed. A strong PA workflow verifies benefits, confirms PA requirements, assembles the clinical documentation packet, submits the request through the payer’s preferred channel, follows up until a decision is issued, documents approval numbers/effective dates, and manages denials or appeals when needed.
Table of Contents
What Is Prior Authorization?
Prior authorization is a payer requirement to obtain approval before delivering certain services. The goal is to confirm medical necessity and coverage rules in advance so the clinic can reduce avoidable denials and patient billing surprises.
Requirements vary by payer, plan type, and service. Some services require PA for every case, while others require PA only for specific diagnoses, frequency limits, or high-cost items.
Prior Authorization vs. Referral vs. Precertification
| Term | What it usually means | Who initiates | Key output |
|---|---|---|---|
| Prior authorization | Plan approval required before a service is performed | Provider/staff (sometimes patient) | Authorization number + approved dates/units |
| Referral | Primary care direction to see a specialist (plan rule) | Referring provider | Referral record or number (plan-specific) |
| Precertification / pre-approval | Often used interchangeably with prior authorization | Provider or staff | Approval confirmation (plan-specific) |
When Prior Authorization Is Required
Common categories that often require PA include advanced imaging, high-cost procedures, outpatient surgeries, DME, specialty injections, and some therapies. The correct answer always depends on the patient’s plan benefits and the payer’s current utilization management rules.
Best practice
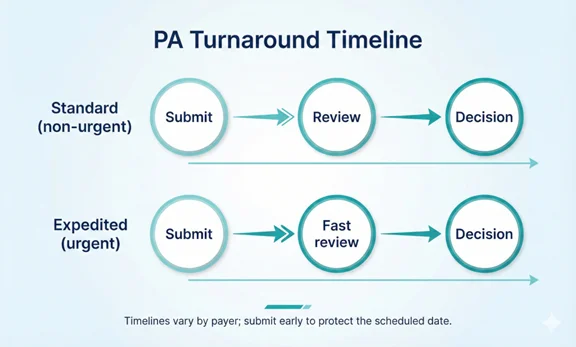
Use a consistent front-end check for every scheduled service: verify eligibility, confirm if PA is required, identify documentation requirements, and submit the request early enough to protect the scheduled date.
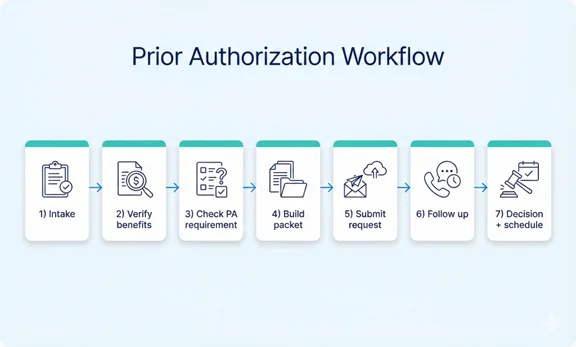
Step-by-Step Prior Authorization Workflow
- Intake (order + scheduling details): Confirm the ordered service, diagnosis, CPT/HCPCS (if known), place of service, rendering provider, and planned date of service.
- Benefits and PA requirement verification: Verify eligibility and benefits, then confirm whether PA is required for the specific service under the patient’s plan.
- Determine documentation requirements: Identify the payer’s clinical criteria and what documents are needed (notes, imaging reports, conservative therapy history, etc.).
- Build the clinical packet: Assemble a complete packet that matches payer requirements. Incomplete packets are a top reason for delays and pending requests.
- Submit the PA request: Submit through the payer’s preferred method (portal, fax, phone, EDI 278, or electronic API workflows where available). Capture confirmation details.
- Follow up and respond to payer requests: Track the request status, respond quickly to requests for additional information, and document all interactions.
- Decision capture and scheduling alignment: Record the authorization number, effective dates, units/visits, and any limitations. Share the outcome with scheduling and clinical teams.
- Denial handling (if needed): If denied, determine whether to correct/resubmit, submit an appeal, or adjust the plan of care based on coverage rules.
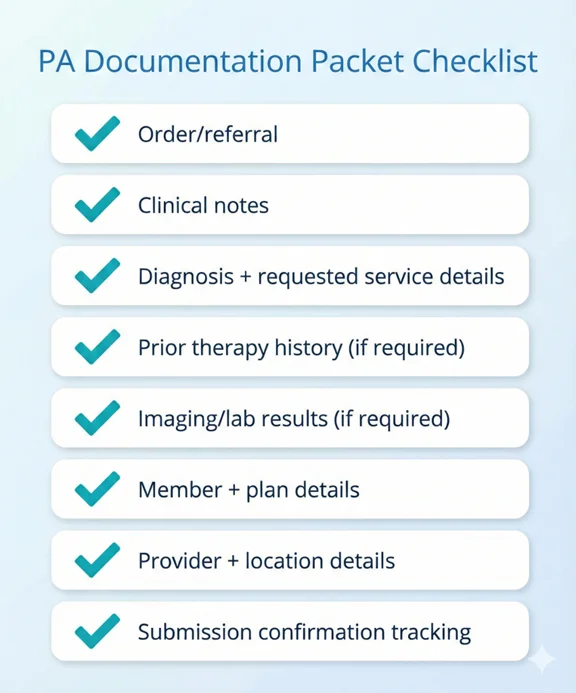
Documentation Packet: What to Include
Documentation varies by payer and service, but most successful PA submissions share a consistent structure.
- Provider order/referral and reason for service
- Relevant clinical notes (history, exam, assessment, plan)
- Diagnosis codes and requested service details (procedure, units, frequency, site)
- Prior conservative therapy history (when relevant) and response to treatment
- Supporting test results (imaging, labs) when required
- Patient demographics and insurance information (member ID, plan, group #)
- Facility/location details and rendering/billing provider identifiers
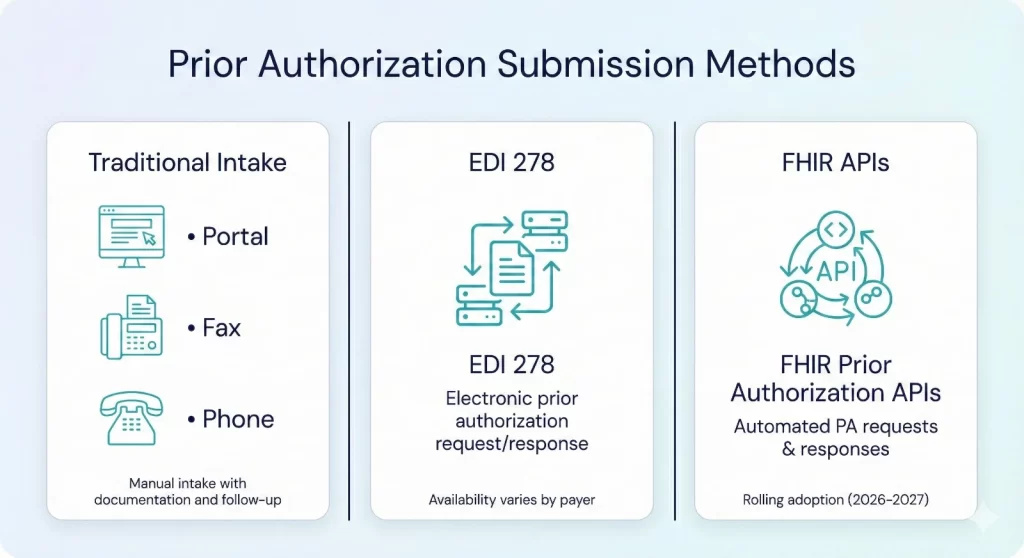
Submission Methods (Portal, Fax, EDI 278, APIs)
Portal / fax / phone
Many payers still rely on portals, fax submissions, or phone-based intake for PA. These methods require strong documentation, timestamps, and follow-up discipline.
EDI 278 (prior authorization transaction)
In HIPAA EDI environments, the X12 278 transaction set can be used for health care services review requests and responses (often associated with prior authorization). Adoption and payer readiness vary, so clinics often need multiple submission paths.
FHIR-based prior authorization APIs (where available)
CMS has finalized requirements for impacted payers to implement a Prior Authorization API that supports PA requests/responses and communicates approvals, denials with reasons, or requests for more information. These API requirements have compliance dates beginning in 2027, while some PA process requirements begin in 2026 (payer-type dependent).
Follow-Up and Turnaround Time Management
A PA request can be delayed by missing documentation, mismatched service details, or unclear clinical rationale. The fastest programs keep a daily follow-up cadence and use a single tracking board that shows status, deadlines, and next actions.
Practical follow-up controls
- Same-day submission confirmation (portal receipt, fax confirmation, reference number)
- Daily queue review for pended requests or missing information
- Escalation rules for urgent cases and appointments at risk
- Clear documentation of payer criteria, requests, and what was sent
Denials: Resubmissions, Appeals, and Next Steps
When a PA is denied, the next best step depends on the denial reason and whether missing information or different documentation can address it.
Common denial categories (high level)
- Clinical criteria not met (medical necessity)
- Missing documentation or incomplete packet
- Incorrect service details (procedure code, site, units, diagnosis mismatch)
- Out-of-network/provider eligibility issues
- Administrative issues (wrong plan, member details, duplicate request)
Decision pathway (simple)
| Denial reason | Best next step | Goal |
|---|---|---|
| Missing info / incomplete packet | Submit additional information or resubmit a corrected request | Move to approval quickly |
| Administrative mismatch | Correct member, service, or provider data and resubmit | Prevent avoidable repeats |
| Clinical criteria not met | Assess appeal viability and include stronger clinical documentation | Overturn when appropriate |
Renewals and Ongoing Authorizations
Many authorizations have limits (dates, visits, units). Track authorization end dates and usage so renewals are submitted early before the patient’s next scheduled visit.
- Authorization start/end dates
- Units/visits approved and remaining
- Frequency limitations and diagnosis constraints
- Renewal submission window and required updated documentation
KPIs to Track (Weekly/Monthly)
| KPI | What it tells you | Common action |
|---|---|---|
| Average PA turnaround time | How quickly approvals are obtained | Submit earlier, improve packet quality, tighten follow-up cadence |
| First-pass approval rate | Quality of submissions and documentation | Standardize packet templates and train intake checks |
| Pended rate (requests for more info) | Where submissions are incomplete | Add checklists and required-document triggers |
| Denial rate by payer/service | Where criteria or coverage issues occur | Pre-check criteria, adjust documentation, consider alternatives |
| Appointments at risk due to PA | Operational risk to scheduling | Escalate urgent cases and flag deadlines |
Security, Privacy, and Compliance Notes
Prior authorization workflows contain protected health information (PHI). Use secure file sharing, role-based access, least-privilege permissions, and audit trails. Avoid sending clinical documents through insecure channels and ensure vendor access is covered by appropriate agreements.
How Claim N Billing Handles Prior Authorizations
We manage prior authorizations as a tracked workflow: verify requirements, build the packet, submit via the payer’s channel, follow up daily, and document approvals and limits so the clinic can schedule with confidence. When denials happen, we route to the correct path resubmission with missing info, correction of administrative issues, or appeal support.
What you get
- Benefits verification + PA requirement confirmation
- Clinical packet checklist and documentation coordination
- Submission tracking (reference numbers, receipts, deadlines)
- Daily follow-up and escalation management
- Approval documentation (auth #, dates, units) and renewal tracking
- Denial review and resubmission/appeal support (as appropriate)
Frequently Asked Questions
Ready to Avoid Delays With Faster Authorizations?
Let’s walk through your current workflow and show you how we can support your practice.
Your billing should be as reliable as your care.