
Denial Management & Appeals Services
What is denial management and appeals in medical billing?
Denial management is the process of identifying why a claim was denied, fixing the root cause, and taking the correct next step corrected claim resubmission, documentation submission, or formal appeal so you can recover payment and prevent the denial from repeating. A strong program combines daily denial worklists with clear action rules, fast follow-up, and monthly reporting that turns denial data into prevention improvements.
Table of Contents
What Is Denial Management?
A denial happens when a payer processes a claim and determines it is not payable as submitted. Denial management is the system your clinic uses to: (1) identify the denial reason, (2) decide the correct next action, (3) complete the correction/appeal, (4) follow up until closure, and (5) prevent the same denial pattern from happening again.
The goal is not just to “work denials.” The goal is to reduce preventable denials over time while recovering revenue that would otherwise be lost.
Denials vs. Rejections: Why the Difference Matters
| Type | Where it happens | What it means | Best next step |
|---|---|---|---|
| Rejection | Front-end edits (clearinghouse or payer intake) | Claim was not accepted for processing | Fix the error and resubmit; confirm new acknowledgment |
| Denial | Adjudication (payer processed the claim) | Payer decided the claim is not payable as submitted | Correct and resubmit or appeal, depending on reason and policy |
The Denial Management Workflow (Step-by-Step)
- Capture the denial and route it to the correct queue: Pull denials daily from ERAs/EOBs or payer portals. Route each denial to a worklist based on reason category and urgency.
- Validate claim data and payer policy context: Confirm member details, payer plan rules, dates, codes, authorization/referral requirements, and whether the denial is appealable.
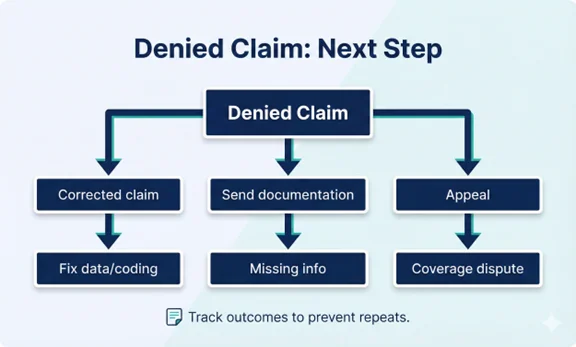
- Decide the correct path: corrected claim vs. documentation vs. appeal: Many denials are resolved by correcting data or submitting missing documentation. Others require a formal appeal. Use clear rules so work is consistent.
- Execute quickly (correct/resubmit or appeal): Submit corrected claims with proper indicators and references. Build appeal packets with clear letters and supporting documentation.
- Follow up and document every touchpoint: Track submission receipts, call notes, portal updates, and deadlines. Escalate aging/high-dollar denials.
- Close the loop: update root-cause prevention: When denials repeat, fix the upstream process (eligibility checks, front-end intake, documentation templates, coding rules, or authorization workflow).

High-Impact Denial Categories to Track
Tracking a short list of denial categories makes your reporting actionable. Start with these categories, then expand as needed.
- Eligibility/coverage issues (inactive coverage, wrong plan, coordination of benefits)
- Authorization/referral required
- Coding/documentation not supported (medical necessity, missing notes)
- Timely filing / deadline missed
- Duplicate/bundling edits
- Provider or location credentialing/enrollment issues
- Claim missing required fields (when it slips past front-end edits)
- Payment policy issues and underpayments

Corrected Claims vs. Appeals (Which One to Use?)
Not every denial should be appealed. Many denials resolve faster with a corrected claim or missing documentation submission. Appeals are best reserved for disputes where you believe the payer’s decision was incorrect based on coverage policy and documentation.
| Scenario | Best Approach | Goal |
|---|---|---|
| 👤 Demographic / Plan Mismatch | Submit a corrected claim with verified member and plan details | Get the claim payable quickly |
| 📄 Missing Documentation | Submit required documentation and confirm payer receipt | Move the claim to payable status |
| 🛂 Authorization Issue | Submit authorization proof and/or a corrected claim (payer-dependent) | Convert denial into payment |
| ⚕️ Medical Necessity Dispute | File a formal appeal with strong clinical documentation | Overturn the denial |
| 💰 Underpayment | Submit a reconsideration or appeal based on payer contract terms | Recover the payment difference |
Building a Strong Appeal Packet
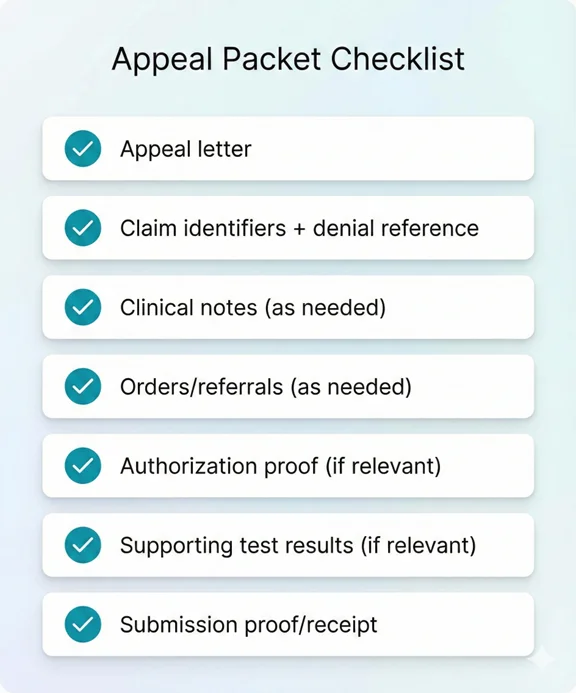
Core appeal packet components (payer-specific)
- Clear appeal letter: what happened, what you’re requesting, and why it should be paid
- Payer claim identifiers and denial references
- Supporting documentation (notes, orders, test results, authorization proof, etc.)
- Corrected claim details (if required) and resubmission indicators
- Proof of timely submission (portal receipt, fax confirmation, certified mail, etc., as used)
Appeal letter structure (simple)
- 1) Patient and claim identifiers (only what’s needed)
- 2) Denial summary and payer reason
- 3) Your rationale (coverage/policy + documentation references)
- 4) Clear request (pay/reprocess/adjust)
- 5) Attachments list
Follow-Up Cadence and Escalation
Denials don’t resolve themselves. A defined follow-up cadence prevents appeal deadlines from being missed and keeps cash moving.
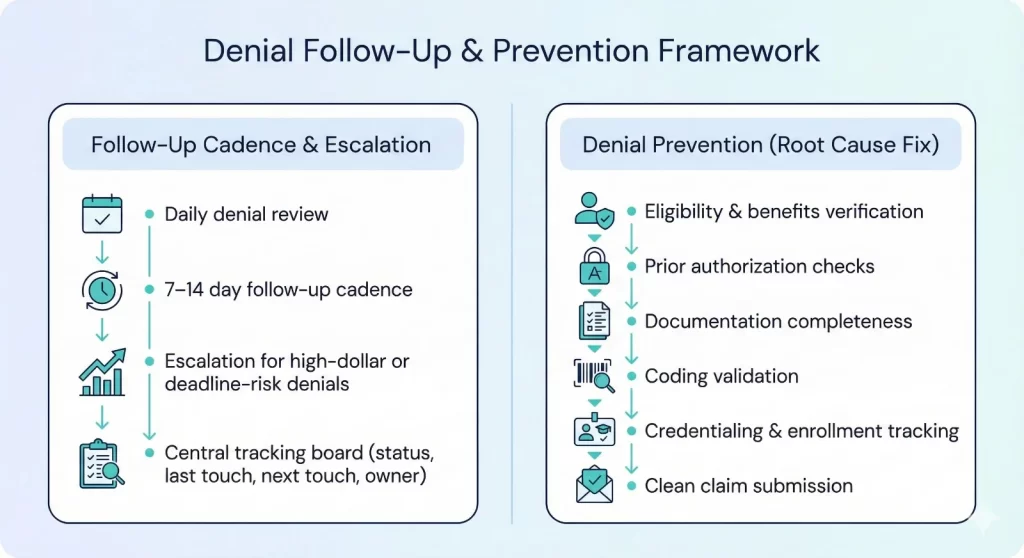
Practical cadence controls
- Daily review of new denials and documentation requests
- Aging-based follow-up schedule (for example, every 7–14 days until resolved)
- Escalation rules for high-dollar denials and deadline risk
- A single tracking board that shows status, last touch, next touch, and owner
Denial Prevention: Fix the Root Cause
The highest ROI denial work is prevention. Use denial trends to improve upstream processes so the same denial doesn’t repeat next month.
Common prevention levers
- Eligibility and benefits checks at scheduling/intake
- Prior authorization verification and packet completeness
- Documentation checklists tied to payer requirements
- Coding validation rules and templates
- Credentialing/enrollment tracking to avoid provider-related denials
- Clean claim submission and fast rejection cleanup
KPIs to Track (Weekly/Monthly)
| KPI | What it tells you | Common action |
|---|---|---|
| Denial rate | How many claims are denied versus processed | Target top denial categories first |
| Preventable denial rate | Portion of denials that could have been avoided | Fix intake, prior authorization, and documentation controls |
| Appeal win rate | Effectiveness of appeal efforts | Improve appeal selection and packet quality |
| Denial turnaround time | Speed from denial receipt to closure | Tighten follow-up cadence |
| Denied-claim A/R aging trend | Cash flow risk tied to unresolved denials | Escalate older and high-dollar denied claims |
Security, Privacy, and Compliance Notes
Denial work often involves clinical notes and sensitive PHI. Use secure file sharing, role-based access, least-privilege permissions, and audit trails. Avoid sending clinical documents through insecure channels and keep vendor access controlled under appropriate agreements and safeguards.
How Claim N Billing Handles Denials & Appeals
We run denial management as a structured system: daily denial intake, clear routing rules, fast corrected claims, disciplined follow-up, and appeal packets built for clarity. We also publish monthly denial trend reports so your clinic can prevent repeats and protect revenue.
What you get
- Daily denial intake and categorization
- Corrected claim resubmissions and documentation submission tracking
- Appeal packet preparation and submission support (payer-specific)
- Follow-up cadence and escalation for aging/high-dollar denials
- Monthly denial trend reporting with prevention recommendations
Frequently Asked Questions
Ready to Recover Revenue From Denied Claims?
Let’s walk through your current workflow and show you how we can support your practice.
Your billing should be as reliable as your care.