Insurance credentialing is the process of enrolling your clinic and providers with payers so you can bill and get paid. In California, most small clinics should plan for 60 to 90 days for Medi Cal enrollment via DHCS PAVE (often longer if anything is missing) and about 60 to 120 days for many commercial payer credentialing decisions once a complete application is in.
If you want credentialing to actually translate into revenue, treat it like a project: build a clean provider file, keep CAQH current, respond to requests fast, and do not start seeing patients “as in network” until you have written confirmation and effective dates.
Why credentialing matters for small clinics
Small clinics feel credentialing in real dollars, not theory.
If you are not credentialed (or you are credentialed but not contracted correctly), you can run into:
- Claims rejecting because the provider is not on file
- Claims denying because the billing NPIs do not match the contracted setup
- Patients showing “in network” expectations that your clinic cannot fulfill
- Delayed effective dates that push revenue out by months
Credentialing is one of the few operational tasks that can quietly decide whether a new location, a new provider, or a new service line becomes profitable this quarter or stalls out.
Credentialing vs contracting vs enrollment (know the difference)
 Small clinics often use one word for three different steps.
Small clinics often use one word for three different steps.
Credentialing
The payer verifies your provider qualifications (license, training, work history, malpractice, sanctions checks). Blue Shield of California, for example, describes credentialing requirements and the need for a complete application with supporting documents.
Contracting
The payer offers terms (rates, fee schedule, participation status, tax structure). You can be credentialed but still not fully contracted for the line of business you intended.
Enrollment
You complete the payer’s enrollment so claims can be submitted correctly (EFT, ERA, pay to details, portal access). For Medi-Cal fee for service enrollment in California, DHCS uses the PAVE portal for enrollment and revalidation actions.
Who needs to be credentialed in a small clinic
Credentialing is not just “the doctor.”
Most payers care about these entities:
- Individual rendering providers (MD, DO, NP, PA, LCSW, LMFT, Psychologist, etc.)
- The clinic entity (group or facility, depending on how you bill)
- Ownership and managing control disclosures where required (common in government programs)
- Service location details (addresses must match exactly across applications)
If any one of these is incomplete, your claims can still fail even if the provider is personally approved.
California credentialing requirements checklist (what you should gather first)
Below is the “clinic credentialing file” we recommend building before you apply anywhere.
Core documents most payers request
| Category |
What you’ll typically need |
Why it matters |
| Identity and licensing |
Current California license, NPI, DEA if applicable |
Payers verify you can legally render the service |
| Work history |
CV with clean timeline and explanations for gaps |
Credentialing reviewers often flag gaps |
| Insurance |
Malpractice certificate of insurance |
Frequently required for network participation |
| Practice info |
Address, phone, hours, taxonomy, services |
Must match across CAQH and payer forms |
| Tax and banking |
W 9, EFT details, pay to address |
Needed for payment setup |
| CAQH profile |
Completed, authorized, attested, maintained |
Many commercial plans pull data from CAQH |
CAQH (commercial credentialing backbone)
CAQH ProView is the industry portal many payers use to collect and re-use provider information. It includes authorization and attestation steps and ongoing maintenance expectations.
Timelines: what small clinics should expect in California
Here are practical planning ranges that match what we see most often when clinics submit complete applications and respond quickly.
Credentialing timeline by payer type (planning ranges)
| Payer type |
Typical timeline |
Notes that impact revenue |
| Medi Cal (CA DHCS) |
Often 60 to 90 days for review, longer if discrepancies |
Start early, especially for new clinics and ownership structures |
| Medicare (PECOS) |
Can be shown as fast as 15 days in some contractor guidance for certain clean PECOS apps |
Development requests, site visits, and risk screens can extend timelines |
| Commercial plans |
Commonly 60 to 120 days after a complete submission |
Many plans rely on CAQH plus payer specific forms |
If a payer tells you “processing,” treat that as a status, not a finish line. Your cash flow timeline starts when you have an effective date you can bill under.
Costs: what credentialing really costs a small clinic
Common cost buckets
| Cost area |
What it includes |
Typical reality for small clinics |
| Provider setup and compliance |
CAQH profile work, document collection, license monitoring |
Time intensive and easy to underestimate |
| Malpractice coverage |
Policy premiums and COI issuance |
Often required before approval |
| Enrollment operations |
EFT, ERA, portal setup, claim testing |
Needed to actually get paid after approval |
| Admin time |
Staff hours, follow ups, resubmissions |
The hidden cost that drags launches |
If you want a clean way to decide “in house vs outsourced,” the question is not just cost. It is: How much revenue do you delay when credentialing drifts by 30 to 90 days?
 For California small clinics, Medi Cal is often the highest impact payer to get right because:
For California small clinics, Medi Cal is often the highest impact payer to get right because:
- Demand is real
- Rules are strict
- Enrollment timelines can push revenue out if you start late
What DHCS PAVE is
DHCS describes PAVE as a web based portal used to submit Medi-Cal enrollment applications, report changes, and respond to revalidation requests.
Medi-Cal timeline planning
A California enrollment resource notes that the PAVE review window typically ranges from 60 to 90 days, and can take longer when discrepancies are found.
Practical Medi-Cal tips that prevent delays
- Make sure service locations, ownership details, and NPIs match everywhere
- Upload clean, legible documents in the format requested
- Respond quickly to DHCS requests for clarification
- Plan your scheduling and marketing so you are not promising “Medi Cal accepted” before effective dates are confirmed
Commercial payer credentialing for small clinics (Blue Shield example)
Commercial plans often run on two tracks: a CAQH driven credentialing review plus payer specific contracting paperwork.
Blue Shield of California’s provider guidance emphasizes that credentialing requires a completed network application with supporting documents, and that the process involves contracting and credentialing steps.
What commercial payers commonly look for
- Complete and attested CAQH profile
- Malpractice coverage and clean work history documentation
- Clear clinic demographics and billing structure
- No mismatches between tax ID, group NPI, and pay to details
The biggest credentialing challenges for small clinics (and how to avoid them)

Challenge 1: Incomplete applications
Small clinics are busy. Credentialing punishes “we’ll finish it later.” Missing documents are one of the most common reasons credentialing stalls.
Fix: build a standardized credentialing packet and reuse it for every payer.
Challenge 2: Entity structure confusion
Group vs individual billing, pay to vs service location, tax ID setup: these details matter. If they do not align, your claims can be rejected even after “approval.”
Fix: map your billing structure before you apply and keep it consistent across payers.
Challenge 3: Delayed effective dates
Even after approval, effective dates decide when you can bill as participating. A delay here is a direct revenue delay.
Fix: track milestones weekly and follow up before a file goes cold.
Credentialing workflow for small clinics (a practical step by step)
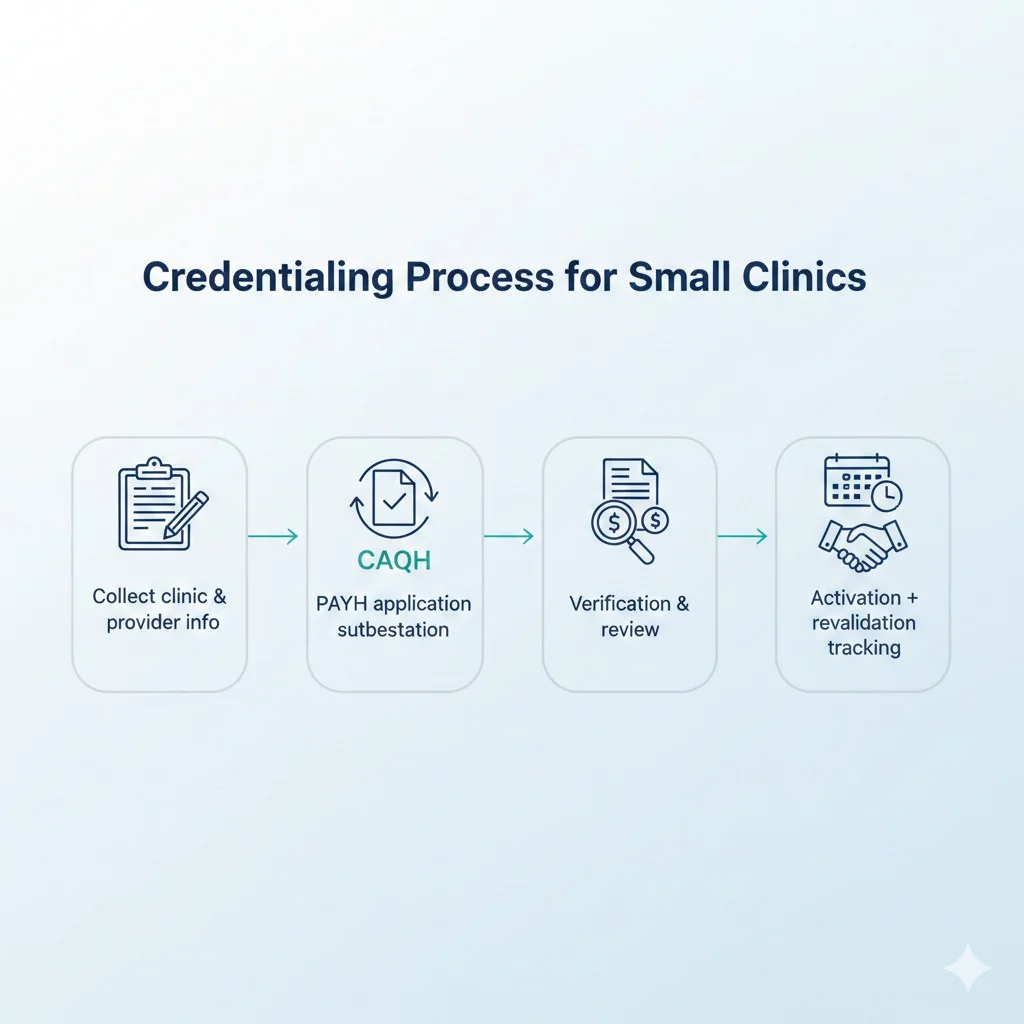
Step 1: Build your credentialing file
Collect licenses, malpractice, CV, NPIs, W 9, clinic demographics, and ownership details.
Step 2: Complete CAQH ProView
Enter the data carefully, upload documents, authorize payers, and attest.
Step 3: Submit payer specific applications
For Medi Cal, apply through DHCS PAVE.
For Medicare, submit via PECOS when applicable.
For commercial plans, follow payer intake instructions and any network applications.
Step 4: Track, follow up, and respond fast
Credentialing is not “submit and wait.” It is a follow up process.
Step 5: Confirm approval and effective dates, then activate billing
Set up EFT and ERA, confirm portal access, and test claims so your first billing cycle does not turn into a denial cycle.
FAQs about Insurance credentialing for small clinics
How Claim N Billing helps small clinics with insurance credentialing
Insurance credentialing can be straightforward on paper and messy in real life. Small clinics usually come to us after they have lost weeks to back and forth emails, mismatched provider data, or payer requests they did not even realize were time sensitive.
With Claim N Billing, our credentialing support is built for small to mid sized practices that need this handled cleanly, with visibility:
- We organize your provider and clinic file so every payer submission is consistent
- We complete and maintain CAQH so commercial credentialing does not stall
- We submit and track Medi Cal enrollment through the DHCS process and respond to requests through the proper channels
- We keep you updated on where each application stands, what is pending, and what the next milestone is
If you are adding a provider, opening a second location, or finally getting serious about being in network, credentialing is the foundation. When it is done right, your billing becomes predictable. When it is done halfway, it becomes a denial factory.
If you want Claim N Billing to handle your credentialing, reach out through using below button and tell us your clinic type, your payers, and your target go live date. We will map the timeline, the required documents, and the fastest clean path to approval.
